However, longer follow-up studies have demonstrated some abnormalities in the proximal femur. Triangular metaphyseal fragment in inferior femoral neck with associated inverted Y appearance 4. While the diagnosis of compartment syndrome is ultimately made based on careful clinical assessments, measurement of compartment pressures is sometimes useful to confirm the diagnosis (174). A Steinmann pin heavy enough to control the proximal fragment is then drilled into the proximal fragment. In obviously displaced fractures, there is no need to perform an arthrogram, and one should proceed directly to open reduction. Resection of a calcaneonavicular coalition with muscle or fat interposition is indicated in a patient younger than 16 years of age who has a cartilaginous bar with no other coalitions present and no degenerative arthrosis, and who has undergone unsuccessful nonsurgical treatment (513, 514). It is essential for intertrochanteric osteotomies in the older child, however, because the mechanical effects are greater, the potential for remodeling is less, and derangements are more complex. Neither the neck-shaft angle nor the head-shaft angle provides an accurate reflection of the severity of the deformity and its likely progression or correction (24, 29). Semitendinosus Tenodesis of Patella for Recurrent Dislocation: the Galeazzi Procedure. Some authors have had success correcting moderate contractures using a simple V-Y advancement of the quadriceps tendon (193, 194). The trochanter and the proximal fragment are pulled down and laterally to displace the proximal fragment onto the diaphysis. Lateral deviation, or orientation, of the articular cartilage may exist, thereby effectively creating a very distal valgus deformity of the metatarsal. Internal polycentric knees move around a center of rotation that varies with the flexion angle of the lower shank (213). It was decided to correct these problems with an innominate osteotomy, as described by Salter. More about the indications and selection of knee joints is discussed later in this chapter. Closing-wedge technique for immediate correction is less likely to stretch the peroneal nerve than opening wedge. Restoration of normal growth in the medial tibial physis is less likely to occur if surgery is delayed such as until 5 years of age (78). The varus derotation osteotomy is used alone in such cases by surgeons who think that redirection of the femoral head toward the center of the acetabulum stimulates normal acetabular development (156, 184, 208, 393ʹ02). Controversy also exists about the amount of weight applied, the direction of application of the force, and the duration of applied traction. When a bending force is applied to a long bone in the immature individual, some of that force is first dissipated in the initial elastic deformity that occurs. Tightness and contractility of the muscles Although there are a number of classification systems in use, two of them seem to be of particular value in attempting to classify clubfeet at the initiation of treatment. However, it is also apparent from such long-term studies that a significant number of patients develop back and knee pain along with radiographic signs of osteoarthritis, with onset decades after the arthrodesis. In preparation for placement of the seating chisel, the site where it will enter the bone is selected. If an open reduction is performed at the same time, the hip is immobilized in accordance with the treatment for that procedure. Medial/lateral column separation (Third Street operation) for dorsal talonavicular subluxation. The advantages include small scars, thus avoiding unsightly scarring (153, 156, 157). This approach has the advantage of involving only one hospitalization and one definitive operation. Image intensifier control in the faux profil projection allows visualization of the distance of this osteotomy line from the acetabulum as it bisects the posterior column between the posterior acetabulum and the sciatic notch (see inset). With regard to the valgus knee, the deformity usually worsens with growth (36, 80, 89, 90).
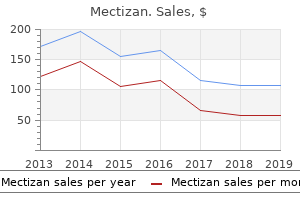
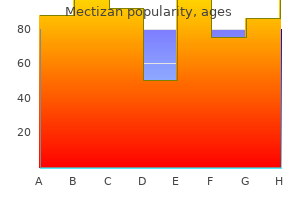
Bioflavonoid Extract (Quercetin). Mectizan.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96317
Partial weight bearing may be resumed in a cooperative child several days after surgery; however, in an uncooperative patient, immobilization in a spica cast for 6 weeks is required. A leg-length discrepancy that refers to discrepancies that are not true differences in anatomic segment lengths are termed apparent or a postural discrepancy. While young athletes have excellent healing potential and regenerative capacities, the apophyses and physes are areas of weakness in young throwers. Plate fixation during and after limb lengthening is another method to decrease fixator time and decrease the incidence of fracture: in contrast to intramedullary fixation, this method can be used in children with open growth plates (205, 206). Motor vehicle accidents (particularly all-terrain vehicles), farm injuries, and gunshot wounds follow in that order (215). In older children and adolescents, complete displacement and 2 cm of shortening are acceptable. B treated with a valgus intertrochanteric osteotomy, especially if it is performed before the child reaches 6 years of age. The need for a period of nonηeight bearing on the affected extremity, when limited internal fixation is used, makes ambulation difficult for these patients. With the blade in place, the plate is rotated toward the shaft, while the shaft is pulled laterally with a large forceps. Men taking anabolic steroids may experience acne, male pattern baldness, priapism, impotence, gynecomastia, and testicular atrophy (10ͱ3). Other risks to this surgery include potential fat embolism syndrome as a result of closed femoral shaft reaming (168). Plastic deformation represents an internal microscopic mechanical failure of bone that results in both an angular and rotational distortion of long bones, seen predominantly in diaphyseal cortical bone. B: Distal osteotomy is required to correct deformity, but proximal femoral shortening osteotomy is additionally chosen due to concerns for weakness from shortening distally. Van Nes (174) later used the procedure for three cases of congenital deficiency of the femur. Historically, resection of a persistently symptomatic talocalcaneal coalition was not popular because of the uncertainty of the outcome (507, 520). A Boyd amputation is suggested for patients with >17 cm of predicted discrepancy or in patients with a nonfunctional foot. B: Long cassette images are used to assess mechanical alignment as well as the anatomic axes of the femur and tibia. In the Chopart partial-foot amputation level, the prosthesis is modified to encompass the calcaneus and talus, and this results in a prosthesis that is often longer than the contralateral limb. The more immature the patient at the time of entering the reossification stage, the greater the potential for remodeling. Sutures can be passed through the free end of both halves to act as handles to aid with later repair. In patients who have the disorder at a young age, the shortness in stature tends to correct during adolescence, whereas patients who have the disorder at an older age tend to be small throughout life (33). Bucholz and Ogden (524) and Kalamchi and MacEwen (528) identified a lateral physeal arrest pattern that may not be evident until a patient is older than 12. The role of bone scintigraphy in the diagnosis of transient synovitis and in the decision making about the management of the condition remains undetermined, and its routine use is not recommended. Advocates of this approach claim that its advantages include minimal soft-tissue dissection, direct access to the medial joint capsule and the iliopsoas tendon, avoidance of damage to the iliac apophysis and abductor muscles, minimal blood loss, and excellent cosmesis. Patients with atraumatic dislocations classically do not recall a specific traumatic event. Given enough time, some of this acetabu- lar cartilage may resume normal ossification and correct a large amount of the dysplasia. Over the years, this modality has been replaced by more promising surgical interventions and is now rarely used by pediatric orthopaedic surgeons.
Remodeling of the femoral neck after in situ pinning for slipped capital femoral epiphysis. With the posterior tibial tendon detached, it is easy to identify the talonavicular joint in a normal foot. Lengthening of congenital below-elbow amputation stumps by the Ilizarov technique. A straight incision is made in the periosteum dorsally, laterally, and plantarward. A lateral view helps identify whether lesions are on the external flexion surface and can show features consistent with normal, benign accessory ossification centers. However, for more proximal lawnmower injuries that will require vascular and nerve repair, along with bone reconstruction and free tissue transfer, the decision needs to be made more realistically. A cartilaginous coalition has the appearance of an articulation with somewhat undulating subchondral bone surfaces. A: Widening and irregularity of the physeal plate are present in the right shoulder. Transtrochanteric anterior rotational osteotomy for idiopathic and steroid-induced necrosis of the femoral head. Conservative measures will relieve symptoms without correcting deformity in most patients with juvenile hallux valgus. Casting usually involves the placing of a casting sock on the residual limb, marking all landmarks and wrapping circumferentially with plaster or synthetic bandage. To correct this deformity, a laterally based wedge of bone is removed from each of the joints to be resected. Workup for systemic causes of pathologic fractures is based on the specific condition that is being considered. In almost all cases of recurrent shoulder dislocation, the instability is due to a combination of injuries to the labrum including bone or soft-tissue Bankart lesions as well as avulsion and attenuation of the capsule from the anterior glenoid. The results of nonoperative management in children are consistently associated with poor outcomes (162, 163). Epiphyseal cannulated screw fixation of small or comminuted tibial eminence fragments can fail due to inadequate bony purchase or further comminution; in these cases, suture fixation is preferred. C margins of the physis to ensure good contact between the physis and interposition material. Soft-tissue release and resection procedures with or without syndactylization, as described by McElvenny (254) and Farmer (260), are appropriate when the metatarsal is normal. A terminal branch of the medial femoral circumflex artery provides the essential blood supply for most of the lateral three-quarters of the femoral capital epiphysis. If the patient is skeletally mature, with no remaining iliac apophysis, it is useful to osteotomize a 1. The duplicate toe may be entirely separate, or there may be simple or complex syndactyly. Persistence of an adduction contracture is always associated with a serious femoral head deformity and will not respond to bed rest or to bed rest with traction (145). A new method of immobilization after traumatic anterior dislocation of the shoulder: a preliminary study. Early deterioration after modified rotational acetabular osteotomy for the dysplastic hip. Surgical treatment is therefore recommended and is most commonly performed with cannulated compression screws. In this age group, hand and elbow radiographs were found to be effective in determining bone age (4, 107). Surgical treatment of an intact pathologic anterolaterally bowed tibia in the infant and/or young child should be avoided. Postoperative ambulation is begun 48 to 72 hours after surgery, once the drains have been removed.

The knees and hips can be flexed 90 degrees and any difference in knee heights recorded (Galeazzi sign) will suggest pathology in the femoral segment (hip joint to knee joint). Lateral acetabular growth stimulation following a labral support procedure in Legg-Calve-Perthes disease. Bone scan has been noted to demonstrate decreased activity in the apophysis of the greater trochanter in 47% of hips affected with chondrolysis, a finding that may precede radiographic changes (363). An open or percutaneous adductor tenotomy is usually necessary in these cases because of secondary adduction contracture, and for increasing the "safe zone" (arc of adductionΡbduction in which the hip remains located), thereby lessening the incidence of proximal femoral growth disturbance. Untreated acetabular dysplasia of the hip in the Navajo: a 34 year case series follow up. In two recent articles, there was no difference in redislocation rates between patients treated with surgical repair at the initial dislocation and those treated nonoperatively. In one large series, the complication rate of orthopaedic treatment of exstrophy was 4% (67). L: Satisfactory tibial alignment and stabilization of the pseudarthrosis have been achieved. Complications from the lengthening process include sudden hypertension during lengthening (263Ͳ65), device malfunction, pin failure, pin tract infection, osteomyelitis, premature consolidation, poor bone formation, fracture after device removal, decreased growth of the limb (266, 267), malalignment during lengthening, pain, soft-tissue scaring, muscle tightness leading to joint stiffness contracture, or even dislocation (268, 269). The proximal femur entry site is made lateral and distal to the tip of the greater trochanter. This procedure creates a compensatory deformity, because the primary deformity cannot be primarily corrected. Ischial containment sockets are not normally recommended (unless needed because of hip instability or nondistal weight bearing) because of problems with soft-tissue containment and diapers in infants. Spontaneous resolution of the deformity can occur up to age 4 years (4, 5), and minor residual deformity does not necessarily lead to disability (4, 6). Progressive subluxation can also occur at the ankle joint with lengthening of the tibia. Because curing of fiberglass also generates heat from an exothermic reaction like plaster curing, the dip water should always be at least room temperature or cooler to prevent burns. Recurrence rates are significant after surgery, and the treatment of choice should be watchful waiting and parental reassurance. The technique will vary, on the basis of prosthetist experience, team philosophy, integration of ever-changing technology, and severity of the deficiency. A comparison of microfracture and osteochondral plug transplantation was performed in a randomized prospective study in the knee joint in children, and both groups showed encouraging results. Although bone formation can be routinely expected, the distance a bone can be lengthened depends on soft-tissue factors too. The faster a hydraulic or pneumatic unit is compressed, the faster the energy is released, and this helps to regulate the lower shank of the prosthesis. It is likely that this would also require release of all of the tendons crossing the ankle joint to prevent foot deformity. Next, the chisel for the 90-degree fixation device is inserted perpendicular to the median plane of the body (B). The geographic cuts in the posterior capsule of the tibiotalar and subtalar joints divide the ligaments as shown: the posterior tibiotalar ligament (A), the posterior talofibular ligament (B), the tibiofibular ligament (C), the calcaneofibular ligament (D), and the deltoid ligament (E). The entire fibula is missing, and there is an anterior tibial bow and missing lateral foot rays. Because of the mild nature of the symptoms, most patients do not present for medical attention until weeks or months after the clinical onset of disease. The snapping initially occurs only rarely and does not inhibit participation in sports. These areas may be analogous to the accessory centers of ossification seen in the periphery of the acetabulum. D: Fifty-one years after reduction, when the patient was 53 years of age, the hip is subluxed and shows severe degenerative changes (Iowa Hip Rating, 48 of 100 points). One of the advantages of the anterior Smith-Petersen approach is that the hip is immobilized in a functional position, with minimal hip flexion and some degree of abduction. This author also asks the parents to perform ankle dorsiflexion stretching exercises for at least 1 minute at least three times per day, because equinus is not only the last deformity to achieve correction, but is also the first to recur. The soft-tissue nail fold must be carefully recreated to prevent chronic toenail ingrowth. E: A second excision of the physeal bar along with lateral physeal stapling has resulted in improved alignment.
Other methods of growth arrest include the use of transphyseal screws as originally described by Metaizeau in 1998 (149ͱ51). E: With the knee in 30-degree flexion, the graft is secured to the intermuscular septum and adductor tendon insertion. A combination of external and internal fixation provides the most consistent results. A difference of <30 degrees has been deemed mild, a difference of 30 to 50 degrees moderate, and more than 50 degrees is deemed as severe (125). Numerous classification systems have been proposed in an attempt to predict the natural history and outcome of treatment. They create a reasonably congruous articulation with the talar head, which is further improved over time by the Hueter-Volkmann law. For displaced type 2 and 3 fractures, Wiley and Baxter found a correlation between fracture displacement with measured knee laxity despite good patient function (5, 119). This fracture is uncommon, and there is some controversy as to whether it actually occurs. In cases in which the condyles are absent or there is the need to fit with a transfemoral socket, rotational control is achieved through proper contouring of the socket relative to the femur - the musculature surrounding the femur has a slight triangular shape in a cross-sectional view, with a flatter contour on the lateral surface, especially proximally. The major distinguishing factor between groups A and B is the presence or absence of a viable lateral column of the epiphysis. For the physician, knowing the existence of medical comorbidities and the natural history of the syndrome is necessary for the care of the child. However, it should be stated that the diagnosis of clubfoot in the newborn can and should be based solely on clinical findings. Reduction and fixation are unnecessary, except for the rare instance in which the clavicle is severely displaced in an older adolescent (12). By changing the hardness of the bumper, the prosthetist is able to effectively change the properties of the foot. Rigidity refers to restriction of subtalar joint motion, which can be assessed in several ways. Injection of arthrographic dye through the hardware under fluoroscopic control and bone endoscopy are two ways that have been reported for checking for pin penetration when high-quality radiographic images cannot be obtained intraoperatively (213, 214). Although the results with this technique appear promising, the technique is demanding, complications are common, and its use has been reported in only a few centers. The technique can be used with leverage on the fragment or direct pushing on the fragment. Fractures of the lower limbs in spina bifida cystica: a survey of 44 fractures fin 122 children. Clinical follow-up with assessment for leg-length discrepancy or angular deformity is done yearly for at least 2 years. Nevertheless, the study confirmed what other studies have shown, which is that there are more flatfooted young children than older children and adolescents. Reliable X-ray diagnosis of slipped capital femoral epiphysis by combining the conventional and a new simplified geometrical method. The cuboid ossifies very early and can undergo a closing-wedge osteotomy to improve adductus deformity in the younger child. The most common congenital upper extremity amputation is by far the transverse forearm (below-elbow) amputation, with radial longitudinal deficiency being the nextmost common. This indirect method of measuring leg lengths has been shown to be accurate within 1. With appropriate surveillance studies of each sport, specific risks and patterns of injury associated with different sports can be determined and compared. However, in unilateral cases, x-rays should be ordered to rule out other pathology such as tumor or infection. Although most commonly this is seen as with autosomal dominant inheritance, cases of autosomal recessive inheritance have been reported by several authors (127ͱ29). The closer together these drill tracks are made, the easier the next step will be. Anti-inflammatory medications can be used for a short period of time, and this often results in rapid improvement. While many of these are stable after closed reduction and casting in 90 to 100 degrees of flexion, just over 20% of fractures treated without operative stabilization may be expected to lose reduction and require delayed surgery (50, 51).
Hallux valgus and hallux flexus associated with cerebral palsy: analysis and treatment. The treatment of this less common position is the same as that for extension fractures. The tripod effect (48) accounts for the varus position that the hindfoot must assume during weight bearing due to the fixed pronation of the forefoot. Arthrorisis by means of a subtalar polyethylene peg implant for correction of hindfoot pronation in children. These adolescents also often struggle with routine activities including donning and doffing socks, cutting toenails, riding a bicycle, and climbing stairs. This distally based flap of soft tissues will either act as the interposition material or will cover a free fat graft that can be used as an alternative interposition material. When angulation is >30 degrees or translation is >3 to 5 mm, closed reduction usually should be attempted because anatomic alignment is associated with better outcome. Anderson and Pagnani (224) also reported a preponderance of poor results in young patients at follow-up an average of 5 years after fragment excision. The clavicle connects the shoulder girdle to the axial skeleton at the sternoclavicular joint. It is wise to deflate the tourniquet before closure in order to check the circulation to the flaps and to control the bleeding. Kalamchi (417) has suggested a modification, placing a notch in the posteriorly cut surface of the proximal fragment and inserting the posterior edge of the distal fragment into the notch. Upon referral to a clinic, the child is assessed by the team, and a treatment protocol is established. In addition, prolonged immobilization and bed rest do not influence the radiographic course of the disease (237, 256, 258, 329ͳ31). There are two oval holes on the side plate, which in the smaller two plates accommodate the 3. Although this method of calculating the eventual discrepancy at maturity is clinically valid, the clinician should be aware of the effect that surgical procedures could have on the growth of the limb. By then transferring the peroneus longus to the brevis, additional pure eversion strength is concentrated at the base of the fifth metatarsal. A: There is a subgroup of patients with adolescent Blount disease who are not obese. The acute stage commences with the onset of pain and decreased range of motion caused by an inflammatory response that lasts for 6 to 16 months. The direction of the rotation is determined by the extent of division of the inner cortex on the inner wall of the ilium. The previously inserted 2-mm smooth Steinmann pin is advanced retrograde through the graft and into the posterior calcaneal fragment. High-pitch velocity and showcase participation also increased the risk for injury. In the Van Nes rotationplasty, the limb is rotated 180 degrees, predominantly through the knee arthrodesis, with some additional rotation through the tibia if necessary. Classically, septic arthritis presents with more severe pain and marked limitation of motion of the hip because of the pain. Despite the limitations imposed by hip arthrodesis, this paradigm will probably remain true until technologic advances have solved the problem of loosening in total joint arthroplasty, especially in young, active patients. For prepubescent children, violation of the tibial and femoral physis presents a risk of significant growth disturbance that would require limb lengthening or osteotomy. The incidence of osteochondral fracture following patellar dislocation ranges from 5% to 50% (36ͳ9). There is usually enough length to fit a prosthetic arm and still permit good active elbow motion. Hence, the condition should not be "medicalized," but rather treated within the context of family, home, school, and play, not through clinic visits. In addition, the diaphysis is used to enlarge the proximal end of the femoral neck. Posterior displacement (C), however, increases the amount of coverage because the ilium is wider in its posterior aspect than in its anterior aspect.
Syndromes
In the rare case of chronic ankle instability in the young athlete, ligamentous reconstruction may be necessary. The "approach-withdraw phenomenon" described by Moseley (211) is when the fluoroscopic appearance of the implanted hardware approaches the subchondral bone and then moves away from it. Some physes overlap the edges of their adjacent metaphyses with cup-shaped contours called lappet formations, as in the proximal tibia. The low dose radiation and convenience of minifluoroscopy make that technology desirable. Surgical correction of large length discrepancies in the lower extremities of children and adults. The same patient is seen in (C) at the age of 12, following a Syme amputation and knee arthrodesis with preservation of the proximal tibial physis. The tibia is approached using a straight longitudinal incision just lateral to the tibial crest. The incision is a straight lateral incision that crosses the lateral side of the talonavicular joint and the distal end of the calcaneus. The snapping hip: clinical and imaging findings in transient subluxation of the iliopsoas tendon. In this age group, the treating surgeon must also consider whether to perform concomitant femoral shortening in conjunction with the open reduction. Before proceeding, it is important to ensure that the capsule has been exposed adequately. If there is sufficient growth remaining, the distal femoral deformity may be amenable to hemiepiphyseal stapling. We prefer a screw for larger patients and athletes likely to stress the fracture early, as well as in cases of elbow dislocations to allow early motion. The variety and succession of past implant materials and designs have prevented a validation study from being performed to determine the overall effectiveness of the procedure or even to validate the concept of the procedure (346). The foot is maximally dorsiflexed and everted and the tendon guided into the third cuneiform and secured over the plantar button. Any other patient with tibial deficiency stands to gain much by the various types of surgical treatment. Using a combination of straight and curved osteotomes, the osteotomy is deepened, heading medially and caudally behind the acetabulum. In the operating room, fluoroscopy is most commonly utilized to guide the surgical approach to the bone bridge. These patients usually have not had a formal reduction maneuver and do not have marked pain or dysfunction following their instability episodes. There are multiple anatomic problems to consider: the pseudarthrosis and consequent malalignment, the flexion/ abduction/external rotation soft-tissue contracture, and the bony stability of the femoralΰelvic articulation. C: the blade plate is inserted and the distal fragment internally rotated (to correct the external rotation deformity). Circumferential periosteal release in the treatment of children with leg-length inequality. Ultrasonography was more sensitive than plain films in detecting hip effusion, but ultrasonographic detection of effusion changed the therapeutic approach in only six patients. If a varus intertrochanteric osteotomy is performed in a hip with an already decreased articulotrochanteric distance, with a proximal physeal growth arrest as frequently seen in Perthes disease, or in conjunction with a medial displacement pelvic osteotomy. Harris reported that symptoms of degenerative joint disease associated with radiographic evidence of acetabular dysplasia occurred early in life and that almost 50% of the patients in his series with acetabular dysplasia had their first reconstructive procedure before 60 years of age, with fewer than 5% having their first reconstruction after 60 years of age (219). The Pavlik harness in the treatment of congenital dislocating hip: report on a multicenter study of the European Paediatric Orthopaedic Society. Open reduction for congenital hip dislocation: the risk of avascular necrosis with three different approaches. The fixator is left in place and progressively dynamized until consolidation and cortication of the osteotomy site is complete. Care should be taken to maintain a pick-up or clamp on the tendon to prevent proximal retraction after release.
In addition, the parents can see the various surgical options that might be recommended for their child. A 5-cm lateral incision is made at the mid-shaft of the femur and minimal subperiosteal exposure completed. The thick capsule extends upward above the inverted labrum, from which it is separated by a shallow groove. Slipped capital femoral epiphysis: early mechanical damage to the acetabular cartilage by a prominent femoral metaphysis. A significant varus deformity of the proximal femur may result in significant abductor weakness, with a persistent Trendelenburg gait and fatigue pain with ambulation. If one accepts my definition of a congenital oblique talus as existing on a continuum between a congenital vertical talus and a flexible flatfoot with a short Achilles tendon (but closer to the Treatment. These techniques are only of historical interest, because better techniques with more secure fixation are now available (165). Ball and Sullivan (399) reported a recurrent valgus deformity in 11 of 17 patients or 61%. Treatment options for partial growth arrest vary depending on the location and size of the bony bar, the degree of angulation caused by the bony bridge, and the amount of skeletal growth that remains. There is severe shortening of the femur, and there is complete absence of a femoralΡcetabular articulation. Complete aphalangia (absence of one or more phalanges from all five digits) Intercalary (I) Transverse (-) 1. In cases of resistant medial tibial stress syndrome after 6 to 12 months of nonsurgical management, surgery in the form of release of the investing fascia overlying the medial soleus (the soleus bridge) and division of the medial soleus origin and periosteum may be indicated (339, 347). Another factor in deciding whether to proceed with a percutaneous or open reduction is how much pronation and supination is possible after a closed reduction. Because of the difficulty in viewing such a complex three-dimensional structure as the acetabulum in two dimensions on a radiographic screen, three pins should be used. Rotational profiles are highly variable, particularly in toddlers who have not mastered the basic skills needed for normal walking, which includes just about every child younger than 2 years and many of those who are 2 to 5 years of age (1, 2, 6, 10). Other variables not controlled or comparable between studies include age at the initiation of casting, number and method of casts, age at surgery, type and duration of postoperative cast management, type and duration of postcast splinting, and length of follow-up. A less commonly used technique for shortening the lateral column of the foot and thereby aligning the talonavicular joint is a closing wedge osteotomy of the anterior calcaneus (C). B: Long cassette radiograph demonstrates varus deformity in the distal femur and proximal tibia in a skeletally immature individual. The blade is held perpendicular to the long axis of the body and directed in an anterior to posterior direction. Posterior medial bowing of the tibia is another congenital condition that has also been shown to accompany a leg-length discrepancy as well as calcaneal-valgus feet (19Ͳ1). Berg (446) cautioned against the use of reverse last shoes and Denis-Browne bars for the same reason. The patient is then allowed to roll back on the sandbag, placing the hip in an obliquely elevated position with the buttocks free. Once an obvious pseudarthrosis is established, surgical treatment can be considered. This joint is found by directing the scissors distally toward the first metatarsal between the neck of the talus and the navicular (A). Although it may be firmly attached to the fascia of the medial gastrocnemius, it almost always communicates with the knee joint. Excision of the fibrous nonunion and autogenous bone grafting from the iliac crest with possible fibular osteotomy has been employed successfully in this rare situation (379). In a severe clubfoot that has not responded well to casting, it may not be possible to immediately approximate the edges of the Cincinnati incision with the foot in the fully corrected position without compromising the circulation of the skin. Although pain is seldom reported as a symptom, older children may report a deep ache in the buttock muscles after prolonged exercise. If the lesion is partially detached, the bed should be freshened down to bleeding bone. Supinating the forefoot places the forefoot in proper rotational alignment with the hindfoot, that is, matched supination of the hindfoot and the forefoot.
A proximal lateral hemiepiphysiodesis is performed to prevent recurrent deformity because the medial physis is no longer functional. The articular cartilage is fragmented, with the superficial zone I missing and with necrotic chondrocytes. Subluxation was the primary factor in the development of degenerative joint disease in this group. The internal type, which is still the most poorly understood, has a variety of presumed etiologies, with snapping of the iliopsoas tendon over the iliopectineal eminence (72) or over the femoral head (71) being the most common. Internal derangement of the knee joint due to pathologic synovial folds: the mediopatellar plica syndrome. She is a poor candidate for external fixation due to risks of infection and her severe immunodeficiency. The subluxating or wandering femoral head in developmental dislocation of the hip. It is possible that this remnant will be present, but good active extension will be absent or the remnant will not ossify. Ponseti has documented the high cellular nature of the medial ligaments in the infant clubfoot, and Zimny et al. All elements and components of the deformity must be analyzed clinically and radiographically. The radiographs should be assessed according to the method described by Paley and Tetsworth (110, 111). Fracture of the lateral condyle is the second most common elbow fracture in children. Classification systems for this disease based on radiographic appearance exist (371ͳ73) but have not been particularly useful in clinical management. The residual limbs can manipulate switches for powered prostheses, giving rise to the temptation to find a prosthetic solution to their problem. The pin in the greater trochanter is used at the same time to pull down the proximal fragment, thereby closing the osteotomy. If the fibula is intact, it may be necessary to complete an osteotomy through a separate lateral incision. The osteotomy should start about 1 cm posterior to the capsule of the posterior facet of the subtalar joint. However, the presence of hip or knee pain should be considered as indications for osteotomy (29). J: Clinical photo after bilateral treatment shows satisfactory clinical correction compared to the preoperative photo. If the varus deformity does recur, a repeat valgus-producing femoral osteotomy can be performed. The anterior portion of the extracapsular ring is formed primarily by the lateral femoral circumflex artery. Treatment of these overuse stress reactions is centered on the discontinuation of the offending force or modification of activities until the symptoms of pain subside. The calcaneus is dorsiflexed and vertically aligned, giving it the appearance of posterior truncation. When using the chronologic graphs, they stressed the importance of taking maturity into account. As the physis transitions from a normal horizontal orientation to a more vertical position, this differential growth becomes more evident. As this is an extra-articular fracture and the main purpose of surgery is to restore the origin of the medial elbow ligaments and the flexor-pronator muscle origins, perfect reduction is not needed. Strength and morphology of growth cartilage under the hormonal influence of puberty. When the articular surface is perfectly reduced the metaphyseal portion may be a little off, as plastic deformation may have occurred in the fragment. The patient has undergone an end-to-end synostosis of the tibia and fibula with proximal fibular resection and a modified Boyd amputation with fusion of the calcaneus to the distal fibula.
In patients with proximal discomfort, the examiner should check for referred pain from the patellofemoral region as patients with the terrible triad of femoral anteversion, genu valgum, and pes planus. The main principles of surgical management of a cavus foot are to (a) correct all of the segmental deformities and (b) balance the muscle forces. Through the use of alignment mechanisms in the components, the prosthetist is able to shift, tilt, and rotate the knee and foot in relation to the socket. He postulated that the cause of this condition was an abnormal or delayed osteogenesis. In more advanced stages of the disease, joint debridement alone might not be sufficient. Satisfactory revascularization and reossification occurred in this morbidly obese 8-year-old child following a 1-year period of nonηeight bearing. This is a consensus definition that has been recently adopted in the medical literature (237, 308, 478 480), but has not been officially adopted in medical dictionaries. Positive outcome from this osteotomy related to preserving the length of the first metatarsal and never dorsiflexing the metatarsal head while stabilizing the osteotomy with a screw or K-wire. For young patients with large defects, autologous chondrocyte implantation is an option because at the current time this tissue most closely approximates native hyaline cartilage. The epiphyseal fragment may be nondisplaced or minimally displaced, making diagnosis difficult. The soft tissues are protected by placing two Bennett or similar retractors around the bone. Prophylactic pinning of the contralateral hip in slipped capital femoral epiphysis: evaluation of long-term outcome for the contralateral hip with use of decision analysis. The true incidence figures are not known, but positional calcaneovalgus may be the most common deformity of the foot seen at birth. Errors in technique can lead to failure in obtaining the desired growth modulation. Findings such as corticalization with three cortices visible on two radiographs and the appearance of a medullary cavity are considered to be signs of adequate strength, but the decision to remove the device is still empiric. The posterior tibial tendon can be identified running above the sustentaculum tali. In this case, the "T-ing" of the capsule is very similar to that done in the anterior approach extending from the anteroinferior spine distally. This system is used when children have demonstrated good control and use of their myoelectric prosthesis and can control both the flexors and extensors independently of each other. Epiphysiodesis in slipped capital femoral epiphysis: a comparison of various surgical modalities. The subtalar joint has an axis of motion that is in an oblique plane that is not frontal, sagittal, or coronal, thus creating motions that are best described with the unique terms inversion and eversion. Nonsurgical treatment is only indicated in the patient with bilateral tibial deficiency with active knee extension and acceptable foot position. The disadvantages of innominate osteotomy are the associated risks and cost factors of the surgical procedure and the procedure for pin removal. Once a satisfactory radiographic alignment has been confirmed, it is mandatory to rule out impingement by carrying out passive flexion and abduction. An arthroscopic fluid pump is used at 35 torr in order to prevent excess bleeding and a tourniquet is routinely used. Femoral shaft fractures in children: a prospective study of the overgrowth phenomenon. The most widely used reconstruction method is the Brom repair, a direct repair and imbrication of the anterior talofibular and calcaneofibular ligaments (250). The patient is then ambulated with a three-point, nonηeight-bearing crutch gait for 6 weeks. Six of these patients were treated by epiphysiodesis for an average predicted leg-length discrepancy at maturity of 4 cm. It has been stated that approximately half of affected individuals will experience symptoms from this deformity, generally due to pressure from shoe wear (262). Bowing, although present in infants, is often not noticed until the child begins standing. The first capsular incision extends along the long axis of the femoral neck anterolaterally.